ErgoPractice News – March 2023
By Jin Chang PhD
[email protected]
Summary
Since SurgiTel’s start in 1992, it has been our mission to enhance the work and lives of our clients by supporting their best working posture, alleviating neck and back strains and pains, and protecting their eye health. SurgiTel’s ergonomic loupes and eye-safe LED headlights have greatly improved the careers of clinicians, but they are not the only tools necessary to mitigate working pain.
Ergonomics can be considered like a tripod. A tripod with only two legs cannot support itself, but a three-legged tripod supports itself with ease. Ergonomic loupes are the first leg, and eye-safe LEDs are the second leg. The third leg of the ergonomic tripod is our ergonomic seating, and in conjunction with SurgiTel loupes and lights help you achieve and maintain a correct posture. With seating that allows for multiple adjustments, our stools are designed to fit both you and your work.
Traditional Nonergonomic Stools
Traditional stools have many problems for numerous clinicians. First, the seat pans are too large or too deep, causing many to sit on the edge of the chair, and not utilizing the lumbar support. Second, many seat pans on traditional stools have a very defined, hard edge where the seat pan top meets the edge of the seat, which cuts off the circulation in the back of the leg.1
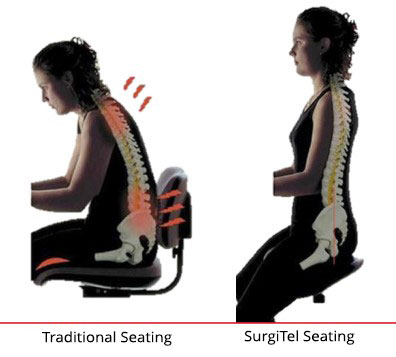
The seat pan largely influences your pelvic position, which is the foundation of your seated posture. The more neutral your pelvic position, the more balanced your spinal curves become, creating less strain in the back, neck, and shoulders.2 Most seat pans are designed so the user’s thighs stay parallel to the floor.1-3 Sitting in this position, with the thighs parallel to the floor, forces the pelvis to rotate up and forward into a non-neutral position. This posture flattens the natural lumbar curve in the spine, doubles the compression on the intervertebral discs in the spine, and forces the back muscles to support the torso, substantially increasing physical fatigue (Figure 1).1,2,7,8
Deep seat pans and low seating positions increase the distance from the clinician to the patient, forcing clinicians to work with outstretched arms, resulting in an arm abduction that creates stress on the entire shoulder girdle.1,4-6
Ergonomic Stools
To offer the best ergonomic seating, SurgiTel is partnered with ergonomic seating experts. There are three types of ergonomic seating, saddle stools (Figure 2a), active seating (Figure 2b), and waterfall seating (Figure 2c). Unlike traditional nonergonomic stools, ergonomic saddle stools allow clinicians to sit tall and up close with the legs spread apart, creating a tripod between the torso and lower limbs.1 Research suggests that the optimal seated posture for operators is hips higher than knees. The increased hip angle decreases muscle activity in the low back, as well as disc pressure.2 As well as having hips higher than knees, clinicians should have their torso as close to the patient as possible, using a seat height that places the patient’s head at waist height. Positioning yourself this way keeps the forearms parallel to the floor and close to the body, favoring a neutral position.1,4-6 It is also important to remember that the spine requires movement to remain healthy, so you should select a stool that allows for frequent spinal movement or readjustment to help reduce low back pain.2,11Active seating options on the stool allow for frequent positional changes during a procedure, minimizing the risk of injury and helping the clinician maintain a neutral and supported posture.12,13 With waterfall seating, the seat is designed to slope downward slightly, relieving pressure on the back of the thighs and offering support to other parts of the legs and back.

For additional support on your ergonomic seating, an armrest can be very beneficial (Figure 2d). Studies have found that using armrests can prevent neck, shoulder, and low back pain. They have also been shown to decrease muscle activity in the neck and shoulders of dentists, especially in the upper trapezius on the dominant side-areas where dentists tend to report a high incidence of pain. Dr. Bethany Valachi found in her lecture test results that approximately 75% of dentists reported decreased or eliminated neck pain when their arms were properly supported.14 As with ergonomic chairs, there are different styles of armrests. A very popular and effective style among general dentists is the movable telescoping armrest which moves in/out and forward/backward with the operator and can be set at a specific height and resistance. Those in professions that work in one position for long periods of time may find that an adjustable fixed armrest provides the best support. While in a fixed position, this type of armrest is highly adjustable in multiple directions: width, height, forward/backward, and in some models, the armrest itself can be tilted for optimal hand positioning.15 Having the armrests properly adjusted to where there is no palpable tension in the operator’s upper trapezius muscles when resting on the armrests is essential to preventing neck and shoulder problems. If the armrests are too high it can actually make neck pain worse, as it can cause neck stiffness and pain at the crook of the neck and shoulder. Proper width adjustment, the space between the armrests, is also important, as armrests that are set too far apart will cause abduction of your arms. Positioning the armrests too far forward can encourage the clinician to lean forward, compromising their ergonomic posture.15
If you’d like to learn more about ergonomic seating, you can read more in our December 2017 issue of ErgoPractice News.
Invest in Your ErgoPractice!
Your stool is just as important to your ergonomic health as your loupes are, and working with SurgiTel to establish the three legs of ergonomics in your career and in your practice is an important investment in more than just your health. For more information, contact your local representative at www.SurgiTel.com/MyRep!
References
- Guignon, Anne N. “Have a Seat: Ergonomic Conversations Turn to Dental Clinician Seating.” RDH Magazine, August 26, 2015. https://www.rdhmag.com/career-profession/students/article/16405433/have-a-seat-ergonomic-conversations-turn-to-dental-clinician-seating.
- Valachi, Bethany. “Operator Stools.” Essay. In Practice Dentistry Pain-Free: Evidence-Based Strategies to Prevent Pain and Extend Your Career, 93–95. Portland, OR: Posturedontics Press, 2008.
- Hayes, Melanie J, Derek R Smith, and Deborah Cockrell. “An International Review of Musculoskeletal Disorders in the Dental Hygiene Profession.” International Dental Journal 60, no. 5 (October 2010): 343–52. https://pubmed.ncbi.nlm.nih.gov/21141207/.
- Mandal, A.C. “The Seated Man (Homo Sedens) the Seated Work Position. Theory and Practice.” Applied Ergonomics 12, no. 1 (March 1981): 19–26. https://doi.org/10.1016/0003-6870(81)90089-2.
- Tiedeman, Jeff. “New Concepts in Seating.” Sitting Comfortably, n.d. http://sitting-comfortably.co.uk/posture%20research%20publications.htm.
- Mandal, A C. “Balanced Sitting Posture on Forward Sloping Seat.” A C Mandal, n.d. http://www.acmandal.com/.
- Harrison, Donald D., Sanghak O. Harrison, Arthur C. Croft, Deed E. Harrison, and Stephan J. Troyanovich. “Sitting Biomechanics Part I: Review of the Literature.” Journal of Manipulative and Physiological Therapeutics 22, no. 9 (November 1999): 594–609. https://doi.org/10.1016/s0161-4754(99)70020-5.
- Karwowski, Waldemar, and William S. Marras. Essay. In The Occupational Ergonomics Handbook. Boca Raton, FL: CRC Press, 1999.
- Snijders, Chris J., Paul F.G. Hermans, Ruud Niesing, Cornelis W. Spoor, and Rob Stoeckart. “The Influence of Slouching and Lumbar Support on Iliolumbar Ligaments, Intervertebral Discs and Sacroiliac Joints.” Clinical Biomechanics 19, no. 4 (2004): 323–29. https://doi.org/10.1016/j.clinbiomech.2004.01.006.
- Kumar, Shrawan. Essay. In Biomechanics in Ergonomics, 32–233. Taylor & Francis, 1999.
- McGill, Stuart. Essay. In Low Back Disorders: Evidence-Based Prevention and Rehabilitation., 175–77. Champaign, IL: Human Kinetics, 2002.
- Chang, Jin. “Don’t Just Treat Your Symptoms, Eliminate the Cause of Your Working Pain.” SurgiTel. ErgoPractice News, December 2017. http://127.0.0.1:8888dont-just-treat-your-symptoms-eliminate-the-cause-of-your-working-pain/.
- “RGP Dental Addresses Ergonomic Factors Affecting Dentistry.” Inside Dentistry. BroadcastMed LLC, April 2009. https://www.aegisdentalnetwork.com/id/2009/04/rgp-dental-addresses-ergonomic-factors-affecting-dentistry.
- Valachi, Bethany. “Answering the Question of Dental Chair Armrests.” Dental Products Report 53, no. 5 (May 2019). https://www.dentalproductsreport.com/view/answering-question-dental-chair-armrests.
- Valachi, Bethany. “Armrests or No Armrests?” Dental Products Report. Dental Products Report, May 25, 2017. https://www.dentalproductsreport.com/view/armrests-or-no-armrests.

